
Page 13 - Demo
P. 13
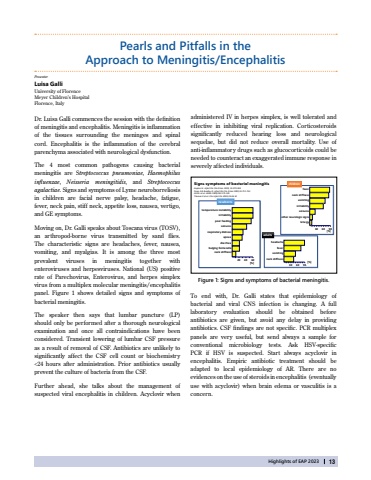
Highlights of EAP 202313Luisa GalliUniversity of FlorenceMeyer Children%u2019s HospitalFlorence, ItalyDr. Luisa Galli commences the session with the definition of meningitis and encephalitis. Meningitis is inflammation of the tissues surrounding the meninges and spinal cord. Encephalitis is the inflammation of the cerebral parenchyma associated with neurological dysfunction.The 4 most common pathogens causing bacterial meningitis are Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis, and Streptococcus agalactiae. Signs and symptoms of Lyme neuroborreliosis in children are facial nerve palsy, headache, fatigue,fever, neck pain, stiff neck, appetite loss, nausea, vertigo, and GE symptoms. Moving on, Dr. Galli speaks about Toscana virus (TOSV), an arthropod-borne virus transmitted by sand flies.The characteristic signs are headaches, fever, nausea, vomiting, and myalgias. It is among the three mostprevalent viruses in meningitis together with enteroviruses and herpesviruses. National (US) positive rate of Parechovirus, Enterovirus, and herpes simplex virus from a multiplex molecular meningitis/encephalitis panel. Figure 1 shows detailed signs and symptoms of bacterial meningitis. The speaker then says that lumbar puncture (LP) should only be performed after a thorough neurological examination and once all contraindications have been considered. Transient lowering of lumbar CSF pressure as a result of removal of CSF. Antibiotics are unlikely to significantly affect the CSF cell count or biochemistry <24 hours after administration. Prior antibiotics usually prevent the culture of bacteria from the CSF.Further ahead, she talks about the management ofsuspected viral encephalitis in children. Acyclovir when Pearls and Pitfalls in theApproach to Meningitis/EncephalitisPresenterTo end with, Dr. Galli states that epidemiology ofbacterial and viral CNS infection is changing. A full laboratory evaluation should be obtained before antibiotics are given, but avoid any delay in providing antibiotics. CSF findings are not specific. PCR multiplex panels are very useful, but send always a sample for conventional microbiology tests. Ask HSV-specificPCR if HSV is suspected. Start always acyclovir in encephalitis. Empiric antibiotic treatment should be adapted to local epidemiology of AR. There are no evidences on the use of steroids in encephalitis (eventually use with acyclovir) when brain edema or vasculitis is a concern.Figure 1: Signs and symptoms of bacterial meningitis.Signs/symptomsof bacterialmeningitisKaplanSL. InfectDis ClinN Am 1999; 13:579594PongA & Bradley JS. InfectDis ClinN Am 1999;13:711-733AttiaJ etal. JAMA 1999;282:175181Thomas E etal. ClinInfectDis2002;35:46-52temperature instabilityirritabilitypoorfeedingseizuresrespiratorydistressapneadiarrheabulging fontanelleneck stiffness204060[%]newbornsfeverneck stiffnessvomitingirritabilityseizuresother neurologicsignsletargy306090[%]childrenheadachefevervomitingneck stiffness306090[%]adultsadministered IV in herpes simplex, is well tolerated and effective in inhibiting viral replication. Corticosteroids significantly reduced hearing loss and neurological sequelae, but did not reduce overall mortality. Use ofanti-inflammatory drugs such as glucocorticoids could be needed to counteract an exaggerated immune response in severely affected individuals.
